Psychomotor Skills Testing… Everything you’ve learned up to this point is now going to be put to the test. For some students (depending on state), you are either at the point that you will now complete your third rides (clinicals), or you’ve completed the course and now you’re ready to graduate.
This is an exciting time because now you get to take all the skills you’ve learned and actually put them to use. But this can also be very scary. For me, it was stressful; however, I was more worried about the written exam. It just depends on if you are a good test taker or if you’re better with hands on skills.
Let’s go over what skills are tested and some important take-aways from each station:
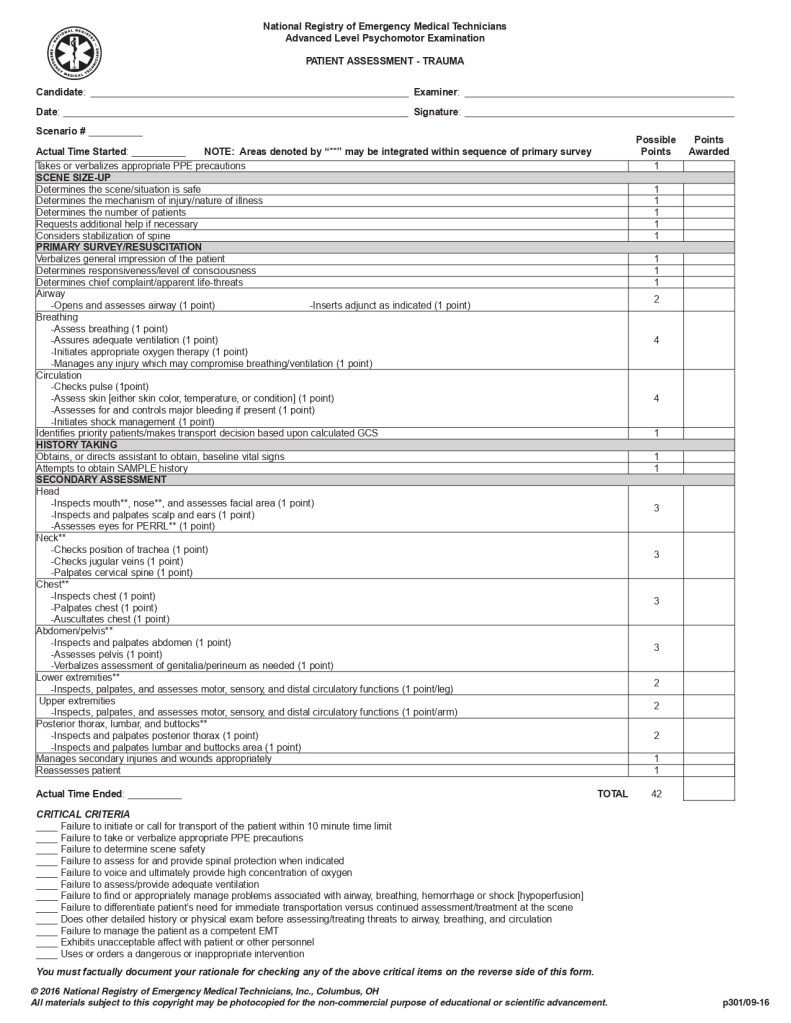
- Advanced Level Trauma Assessment
- This one is similar to your medical assessment, but obviously it’s a trauma call (similar to your EMT/AEMT psychomotor skill station, just with more advanced scope of practice). They’re more than likely won’t be a multi-trauma incident. Make sure you splint/stabilize as needed and get them to the hospital. The big thing here is C-Spine. If there is ANY chance of spinal injury, then just take C-Spine precautions. You can’t lose points for taking C-Spine and back-boarding, so if you’re worried about it, then just do it.
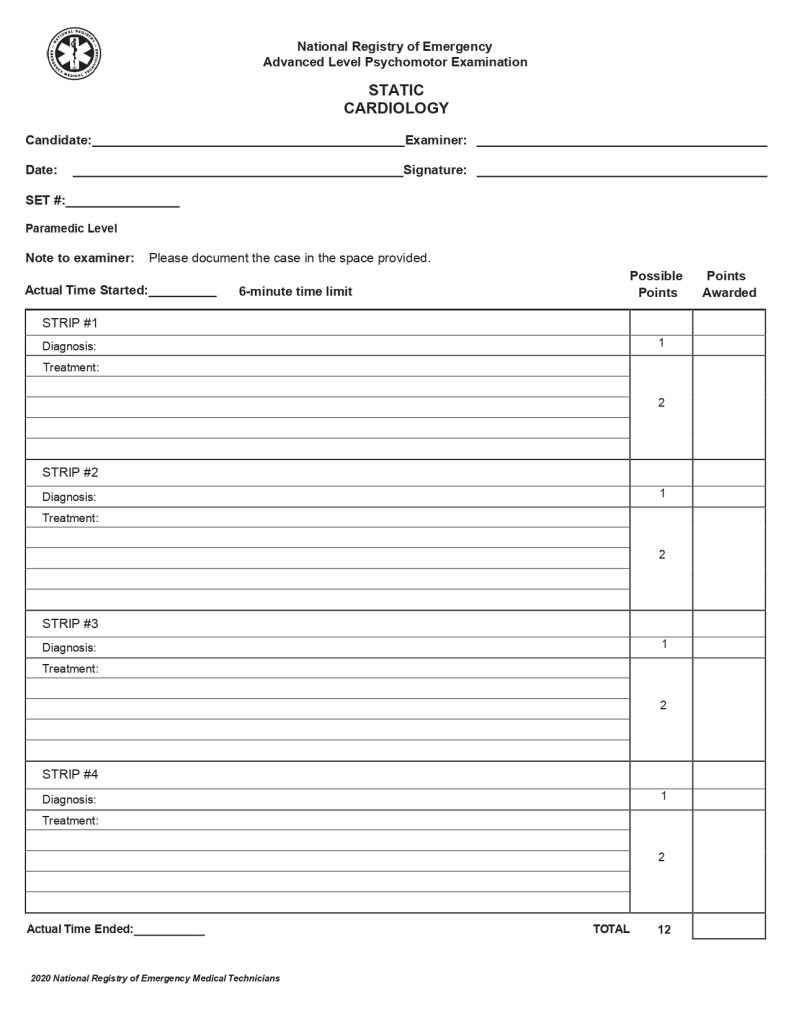
- Static Cardiology
- For this station you will be given ECG rhythms. You will need to identify the rhythm and then state your treatment. Long story short, is the rhythm too fast, too slow, or not enough (cardiac arrest). You will follow the American Heart Association’s Advanced Cardiac Life Support algorithms for each of the four strips that includes: Tachycardia, Bradycardia and Cardiac Arrest. There are no listed “critical fails” for this scenario; however, you do need to identify and treat each patient appropriately within the six minute time limit.
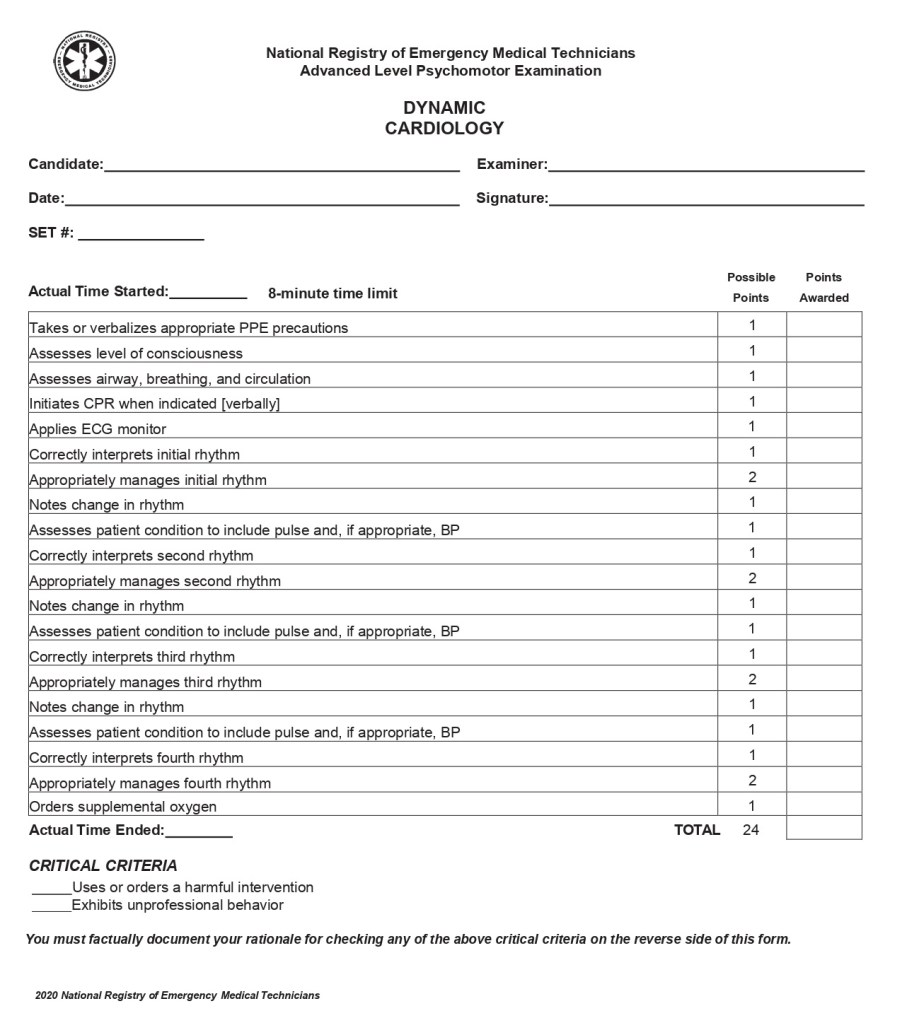
- Dynamic Cardiology
- This station is very similar to the static cardiology station; however, instead of just listing off the rhythm and treatments for the four rhythms, now you will be acting out the station and transitioning through the strips. You will have a cardiac monitor that you will need to apply to the patient and diagnose the patient’s cardiac rhythm. Same as before, is the rhythm too fast, too slow, or not enough? Follow all of the American Heart Association’s Advanced Cardiac Life Support algorithms (tachycardia, bradycardia and cardiac arrest) within the eight minute time limit. The big thing with this scenario is the ability to go between the algorithms seamlessly. Your patient could start off tachycardia; however, after cardioverting them they lose their pulse. Most testing sites will give you a scenario where the patient experiences bradycardia, tachycardia, pulseless ventricular tachycardia/ventricular fibrillation and asystole/pulseless electrical activity.
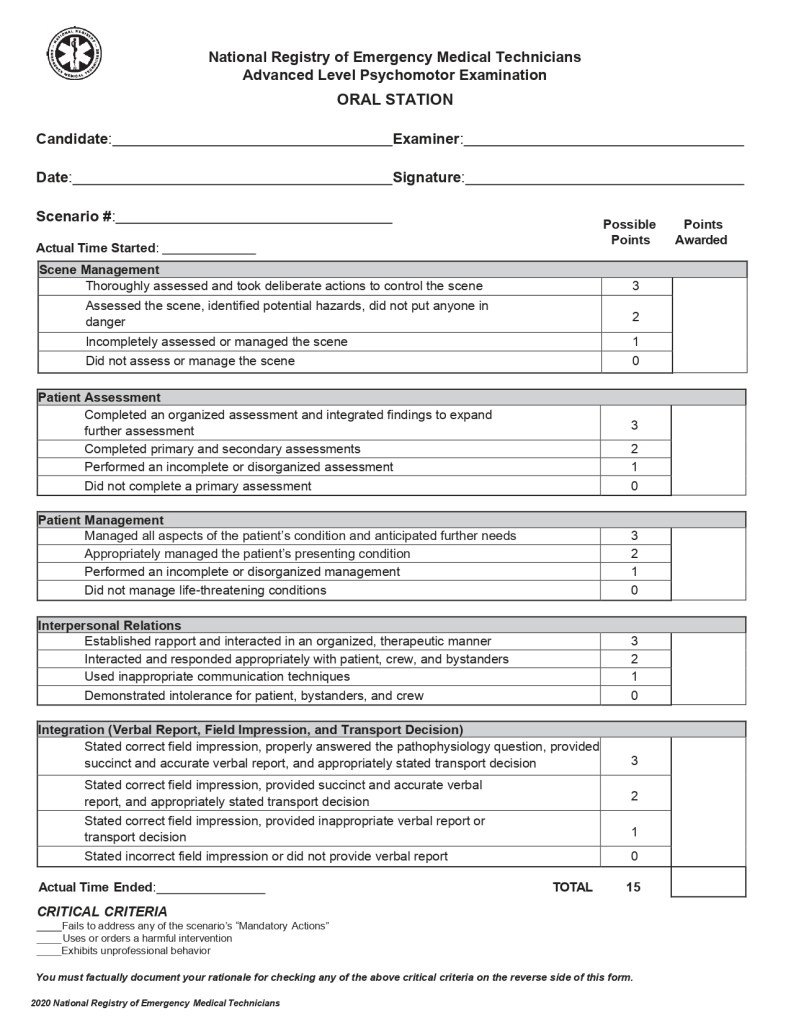
- Oral Station
- The oral station is a medical assessment station where you will talk through the scenario. No skills will actually be performed for this station. Depending on your experience, this could be easier or harder on you. If you have experience, it may be easier for you to “run the call” like this because at some point during your career you have probably run a similar call. Whereas a brand new responder may struggle with this station because they don’t have any experience on the truck quite yet. The grading on this station is pretty loose; you just need to treat the patient accordingly. The biggest thing with this scenario is OVER VERBALIZING EVERYTHING!!! Something as simple as “BSI scene safe” doesn’t cut it with this scenario. When you arrive “on scene,” you will need to ensure the scene is safe. Ask if there are any dogs in the yard, or do you see anyone with weapons, that sort of thing. This skill is all about verbalizing. It sounds cliché, but you can’t over verbalize when it comes to this one.
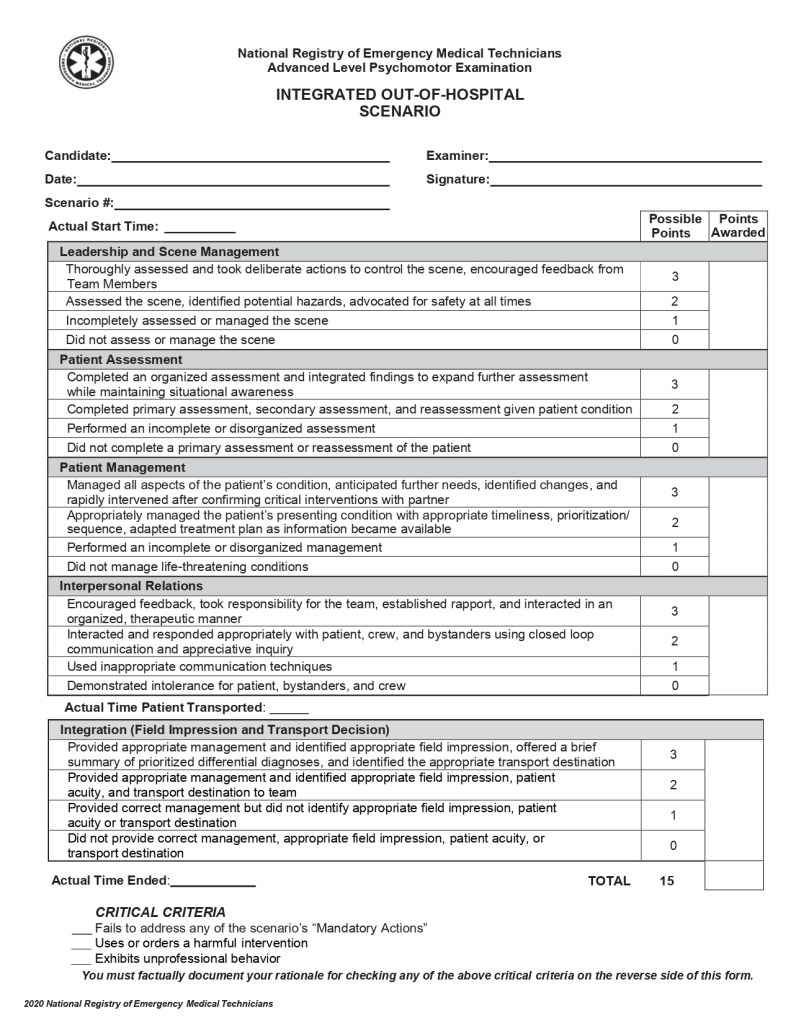
- Integrated Out-of-Hospital Scenario
- This is the fun one… (said no one ever). The out-of-hospital scenario is the scenario that your entire medic school has lead up to. Throughout the paramedic program your instructor has kept a file on all of the skills you have practiced throughout the program. This file is what is known as your “Paramedic Student Portfolio.” This portfolio serves as proof that you were not only trained on every skill, but that you have routinely practiced each skill in accordance with the program requirements. All of these skills are then pulled into this scenario. So instead of testing every skill station as you do for EMT/AEMT, now you are tested on one scenario where a random selection of these skills will be needed. For instance, if you get a motor vehicle collision then you will most likely be required to perform C-Spine, supine spinal immobilization, IV access, and pain management medication administration as needed for the patient. These scenarios are randomized and the skills required change from scenario to scenario. The scenario starts with dispatch information. You will need to request any additional resources and act just like you are running a real call. You will have a partner assigned to you that can act out any skill you ask of them. For this skill, you can’t just say things like “I’ll get a set of vitals,” You will actually attach the patient to your cardiac monitor and take any vital signs that you would like. You will also perform any tasks that need to be completed. This could be anything from starting an IV, to splinting an injury, to intubating a patient. You will arrive on scene, assess, treat, and transport the patient as needed. The worst part of this scenario is the time frame of 20 minutes. Regardless of how long it takes to perform these tasks, you will use the entire 20 minutes. When I tested, I had a child with 3rd degree burns. I had a patient and a mother that I needed to keep calm for that full amount of time. After obtaining vital signs, obtaining IV access, doing the Parkland Formula to determine the fluid resuscitation needed and contacting medical control for 100mcg of Fentanyl, I had 15 minutes remaining. For the remainder of my scenario I had to sit in the “truck” with my patient and his mother. Now this may not seem like it is that big of a deal, but 15 minutes of simulated small-talk is SUPER awkward. For this scenario, I was not only graded on my treatment of the patient, but also on keeping the patient and his mother calm and treating accordingly. Like all of the other skill stations, practice makes perfect!
For more information and examples of these skills stations, I recommend watching the video series by EMTprep on YouTube. For copies of these skill sheets, visit: https://emtprep.com/extra/nremt-exams/nremt-practical-exam-skill-sheets
If you have any questions about these skills stations, or need further explanation please reach out to me using the “Contact Us” page of this site.
