Psychomotor Skills Testing…Everything you’ve learned up to this point is now going to be put to the test. For some students (depending on state), you are either at the point that you will now complete your third rides (clinicals), or you’ve completed the course and now you’re ready to graduate.
This is an exciting time because now you get to take all the skills you’ve learned and actually put them to use. But this can also be very scary. For me, it was stressful; however, I was more worried about the written exam. It just depends on if you are a good test taker or if you’re better with hands on skills.
Let’s go over what skills are tested and some important take-aways from each station:
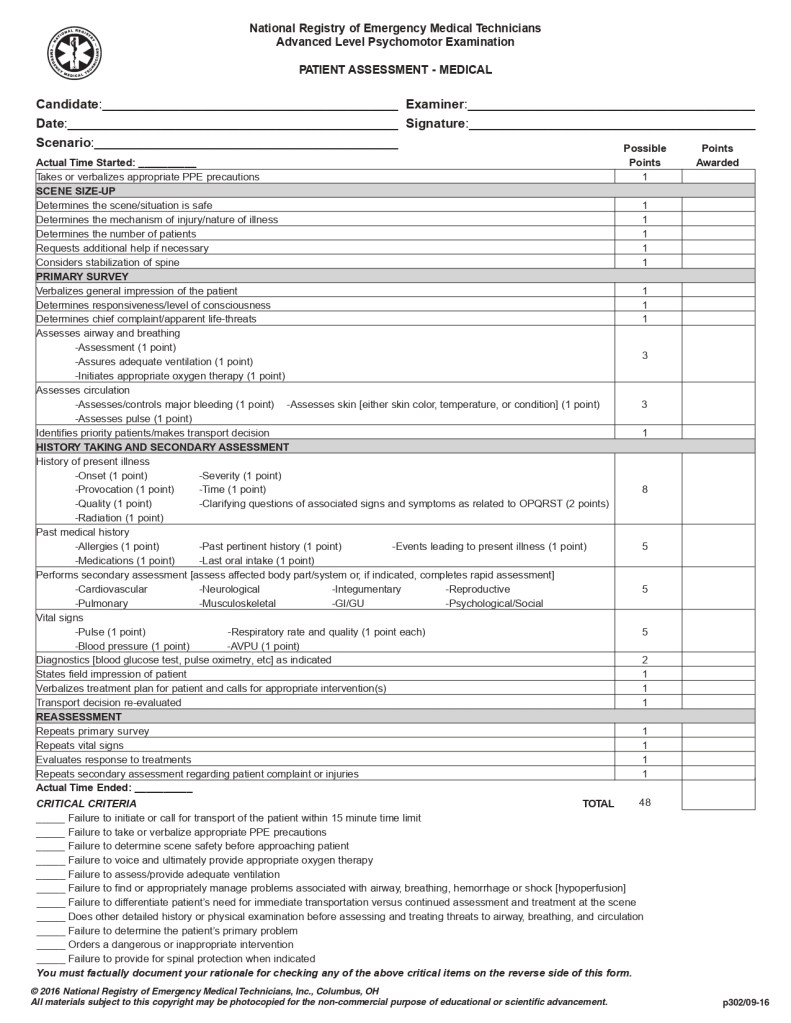
- Advanced Level Medical Assessment
- This is going to be a generic medical complaint (similar to your EMT psychomotor skill station, just with more advanced scope of practice) that you will need to identify and treat. They are not crazy off the wall calls. For the most part, they are straight forward complaints that you will need to identify and treat with the correct medications and dosages. The big ticket item here is being a competent AEMT. If you go into this skill looking like you know what you’re doing, more than likely you will pass with flying colors. Know your treatments, medication indications/contraindications, and dosages.
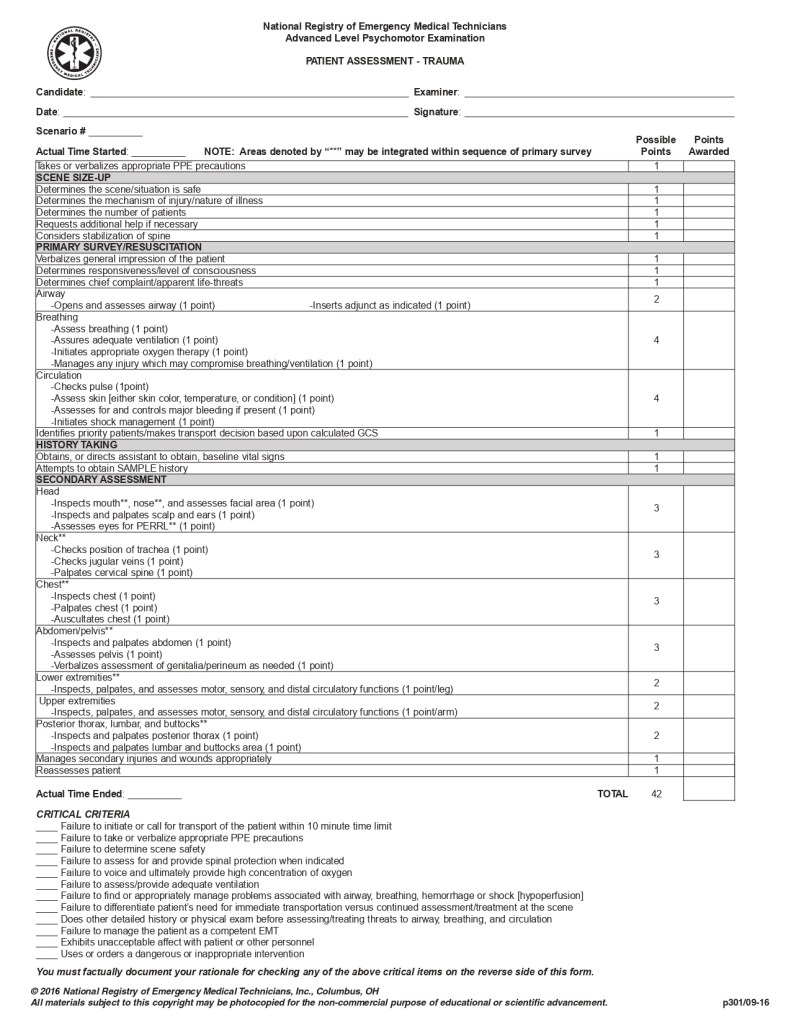
- Advanced Level Trauma Assessment
- This one is similar to your medical assessment, but obviously it’s a trauma call (similar to your EMT psychomotor skill station, just with more advanced scope of practice). They’re more than likely won’t be a multi-trauma incident. Make sure you splint/stabilize as needed and get them to the hospital. The big thing here is C-Spine. If there is ANY chance of spinal injury, then just take C-Spine precautions. You can’t lose points for taking C-Spine and back-boarding, so if you’re worried about it, then just do it.
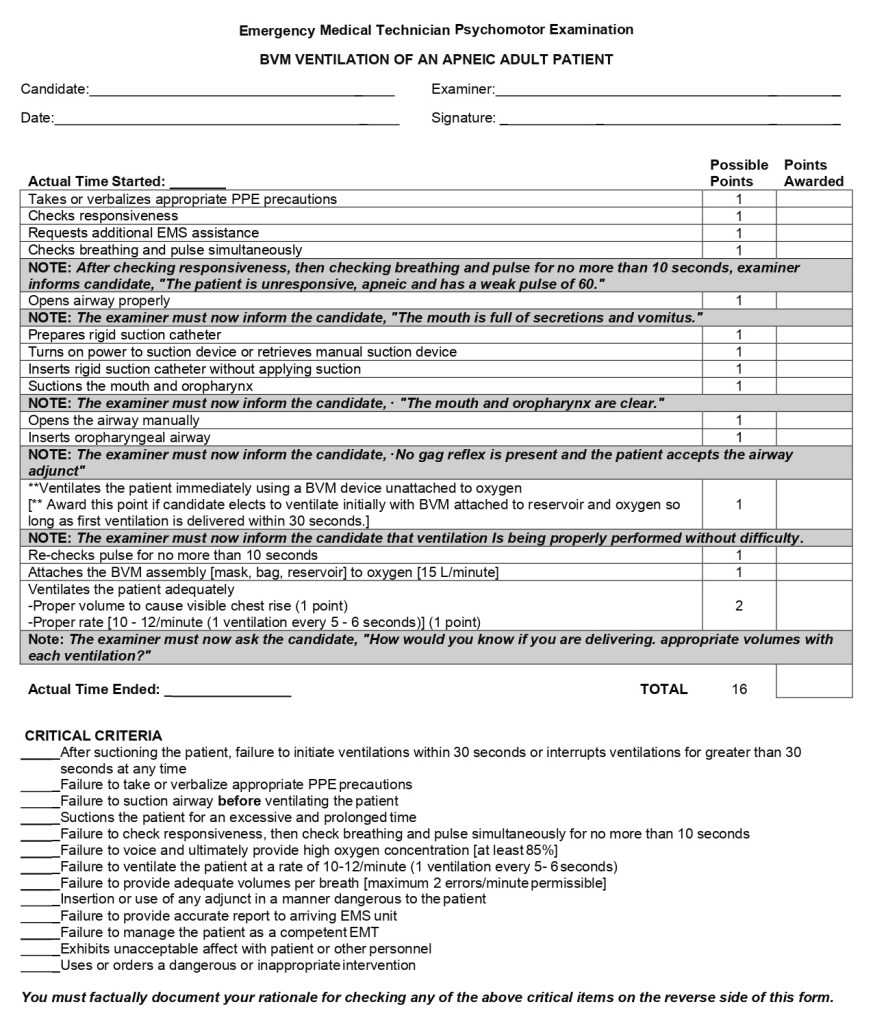
- Bag-Valve-Mask Ventilation of an Apneic Adult Patient
- This skill station you will be assessing a patient who has a pulse but is apneic (not breathing). You will need to open the airway, suction, place an oral pharyngeal airway (OPA) and ventilate with a bag valve mask. Once you ventilate them, you will attach the BVM to oxygen. The big requirement for this skill is that the patient can’t go more than 30 seconds without ventilations after the airway has been suctioned. Once you’ve ventilated them and you are attempting to attach O2, if you have difficulty and are running a risk of going over that 30 seconds, you can always administer another breath to make sure you don’t go past 30 seconds. In my opinion, this is one of the easiest skill stations because it has a TON of prompts from the preceptor. If they don’t give you feedback, then more than likely you have skipped a step.
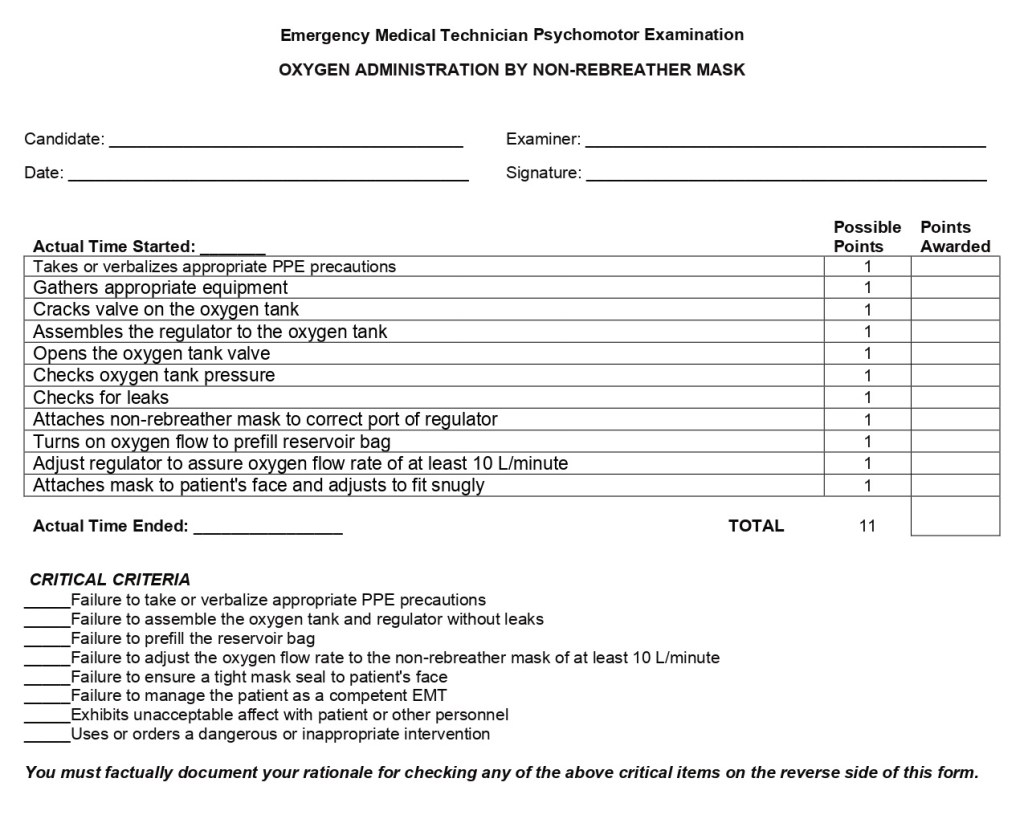
- Oxygen Administration by Non-Rebreather
- This skill station requires you to assemble an oxygen cylinder and regulator and then applying O2 via non-rebreather mask (NRB). Before you attach the regulator, make sure that you “clear the line” by cracking the valve to push out any particles that may be in the port. The biggest critical failure here is making sure that you don’t have any leaks. Make sure that if the regulator doesn’t have a built in O-ring, that you use one otherwise you will have a leak.
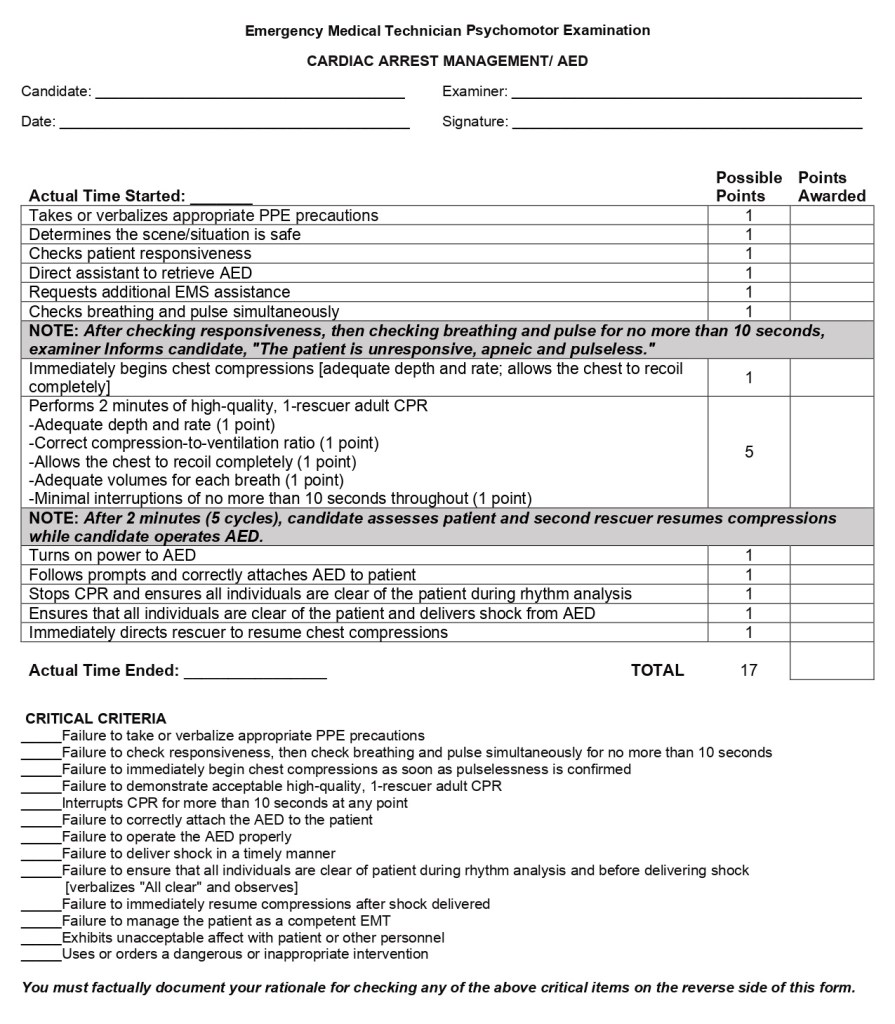
- Cardiac Arrest Management /AED
- This skill follows the current American Heart Association’s Basic Life Support CPR station. As soon as this skill starts, check for a pulse and if they are pulseless, then start CPR at a ratio of 30 compressions to 2 respirations and call for help (and an AED). Once you have completed a cycle of CPR, your “partner” will arrive with the AED and resume compressions. The biggest failure I see with this skill station is not turning the AED prior to attaching the pads. Make sure that you turn on the AED and follow its commands. Failure to do so will trigger a critical fail. So make sure that you turn the AED on prior to applying the pads and plugging in the connector. Also, make sure that following the analysis phase (when the AED says charging) that you resume compressions. Some AEDs will instruct you to stay clear of the patient, but this instruction is for the non-medically trained person, you only want to pause compressions when it is analyzing or delivering a shock. Speaking of shock, make sure you always clear the patient and others from the patient prior to delivering any defibrillation.
One Random Skill Check; including:
For these skills, one will be selected at random for the day of testing. All of the students in attendance will be tested on this same skill. These skills include:
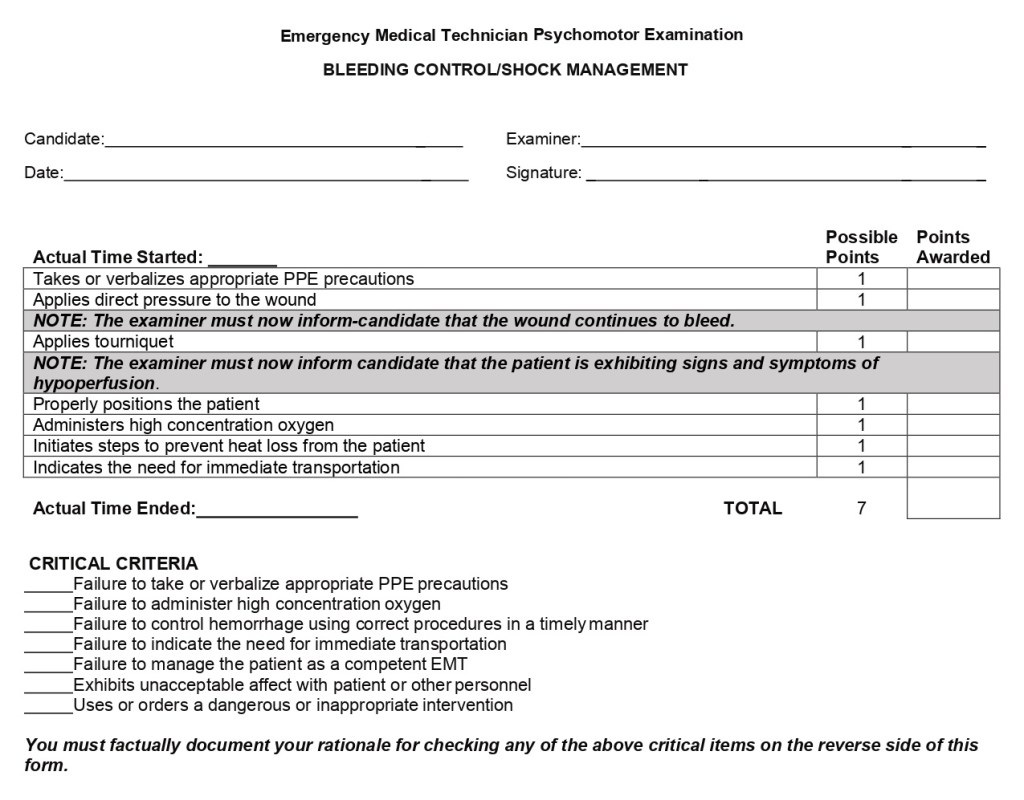
- Bleeding Control/Shock Management
- This one is pretty straight forward and can summarize into: direct pressure, tourniquet, treat for shock, and transport. When it comes to treating for shock, make sure you apply high flow O2, prevent heat loss, and transport immediately.
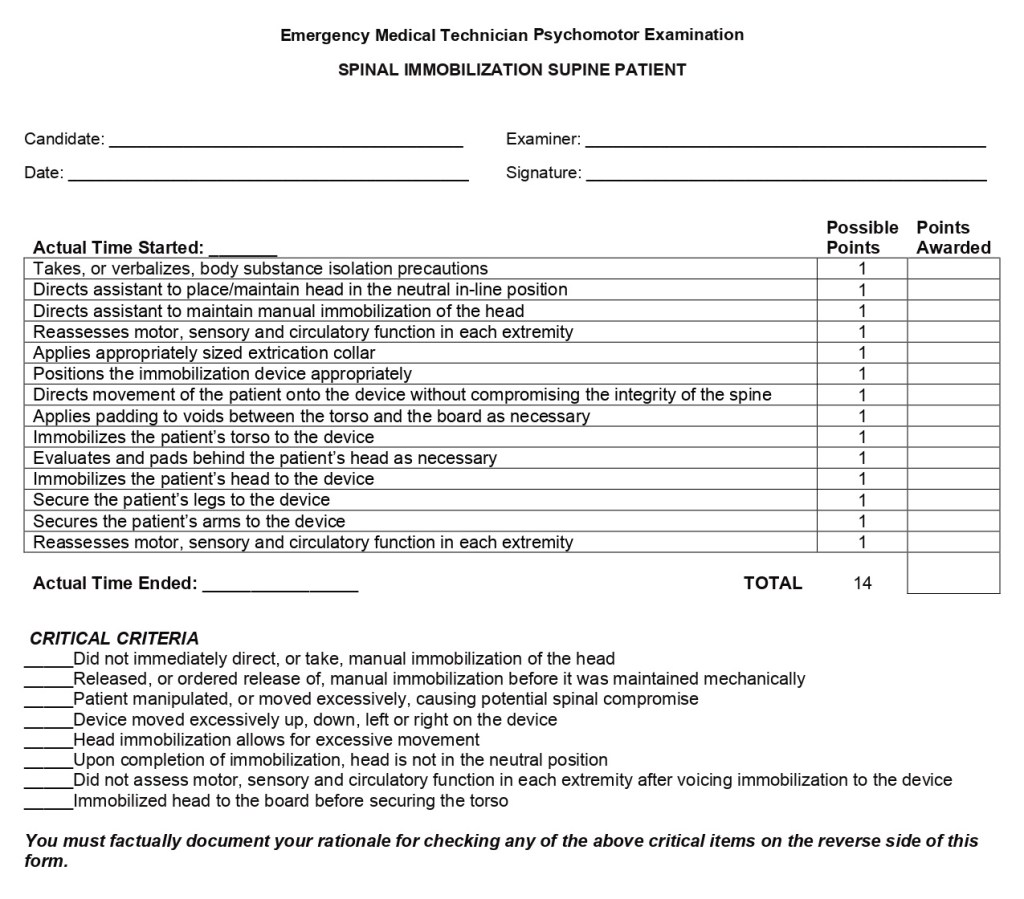
- Spinal Immobilization – Supine
- This skill is pretty straight forward; you will place a patient on a backboard. Make sure you take C-Spine precautions as soon as you ensure scene safety and PPE. Make sure that your “partner” maintains manual C-Spine until the head has been secured to the spinal board (which should be the LAST thing secured). Make sure you also utilize the “Z Method” of moving the patient up or down on the board to minimize movement and pad any voids if needed. You will also want to assess for Pulse, Motor, and Sensory (PMS)/Circulation, Motor, and Sensory (CMS) throughout the treatment. If you don’t ensure this before and after placing them on the board, it is a critical fail.
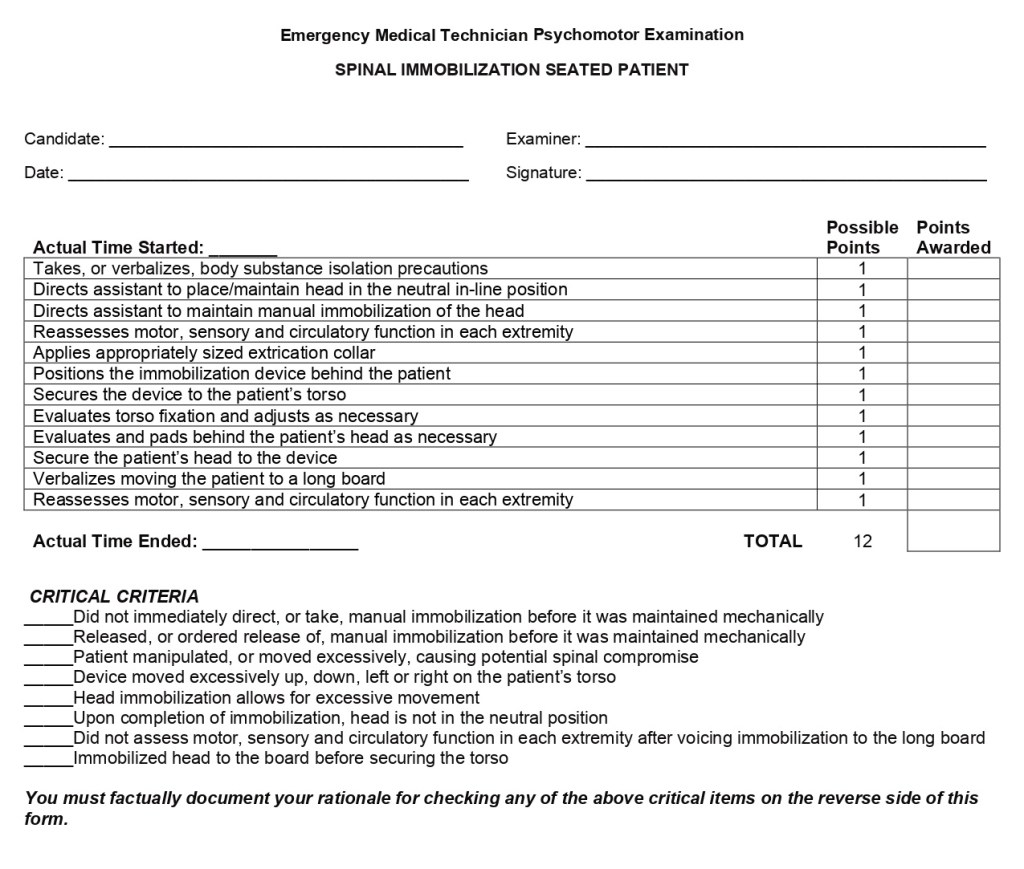
- Spinal Immobilization – Seated
- This skills is nearly a direct “copy and paste” of the supine immobilization; however, you are using a Kendrick Extrication Device (KED) and the patient is sitting up. This station used to require the straps to be secured in a certain order; however, this is no longer the case, as long as the head straps are the last to be secured. As with supine immobilization, make sure that your “partner” does not release C-Spine until the head has been secured. When placing the KED, you want to make sure the device is lifted into the axilla as much as possible to avoid any excessive movement. Also, you want to make sure that all of the straps are snug and as always check PMS/CMS before and after the skill.
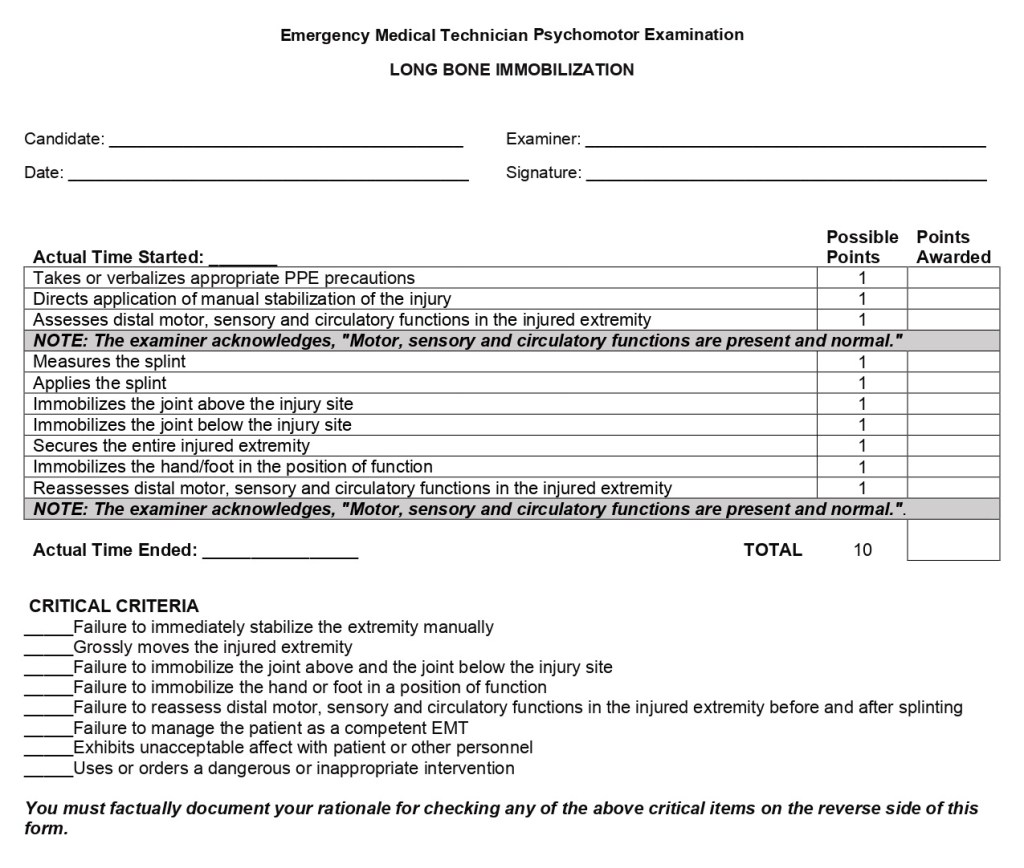
- Long Bone Immobilization or Joint Immobilization
- These skill stations are two different skills; however, they are nearly identical. A long bone could be either a femur fracture or humerus fracture and a joint can be either the knee or the elbow. This is left up to the testing site to choose which random skill station you’ll be tested on, as well as what kind of injury you will be treating. Same as before, you want to check PMS/CMS before and after the skill station to ensure that they remain intact. When splinting, you want to splint against any movement, so it is important that you immobilize above and below the joints above and below the injury. One of the easiest parts to skip with this skill station is to immobilize the hand/foot “in the position of function.” For a hand, this means giving them a rolled package of gauze (or something similar in size) to hold, in a neutral position. For the foot, have the foot facing its normal orientation (if possible) and not flexed outward/inward. If your patient has a possible fracture to their leg, you only apply a traction splint to a MID-LINE FEMUR fracture, again that’s a MID-LINE FEMUR fracture!
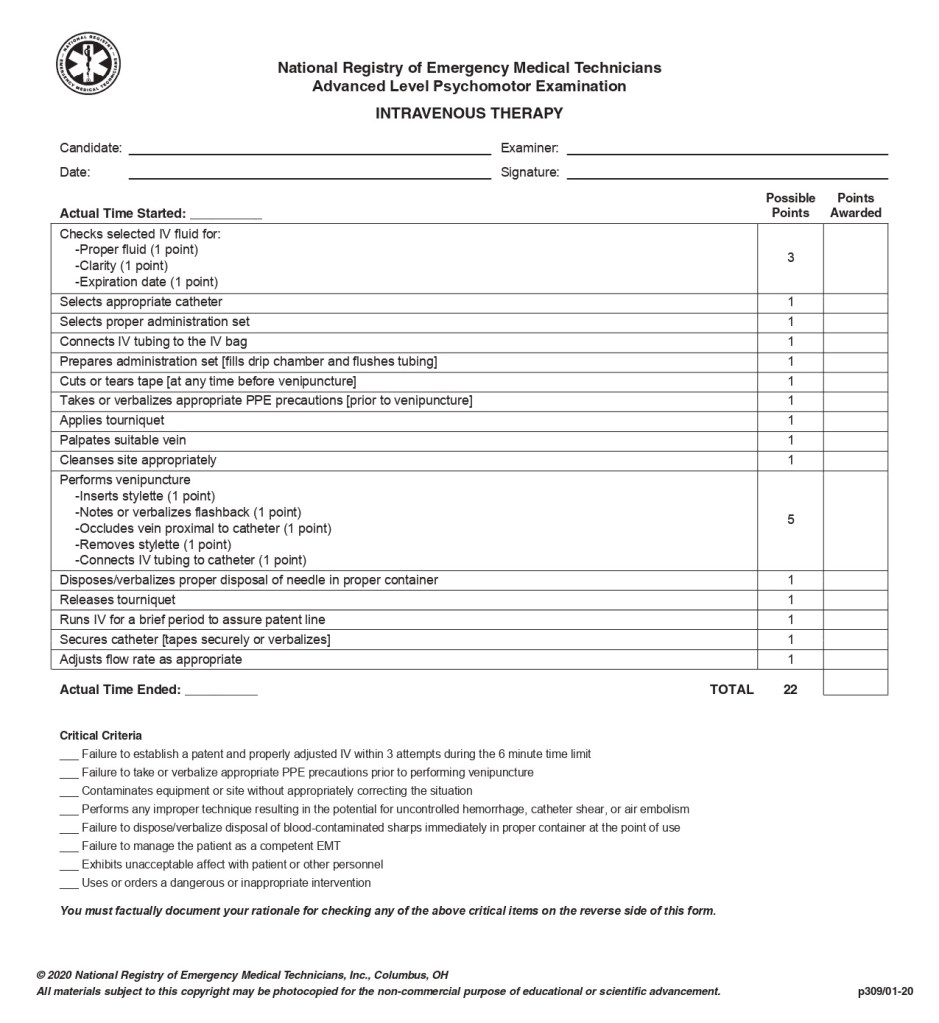
- Intravenous Therapy
- In this skill station you will start an IV and administer fluids. You start off by checking your bag to ensure it’s the correct solution, for clarity, and that it isn’t expired. Make sure that before you puncture the skin that you cleanse the IV site using an “aseptic technique.” What this means is to use an alcohol wipe and wipe in a circular motion outward to ensure that the site is fully cleansed to avoid infection. Once you have “flash,” place a 2×2 under the catheter to soak up any blood that leaks from the catheter prior to placing the INT cap. MAKE SURE YOU DISPOSE OF THE NEEDLE!!! I can’t stress this one enough. In regards to “spiking” the IV bag, ensure that you let all of the air bubbles escape the tubing to avoid causing any complications from administration.
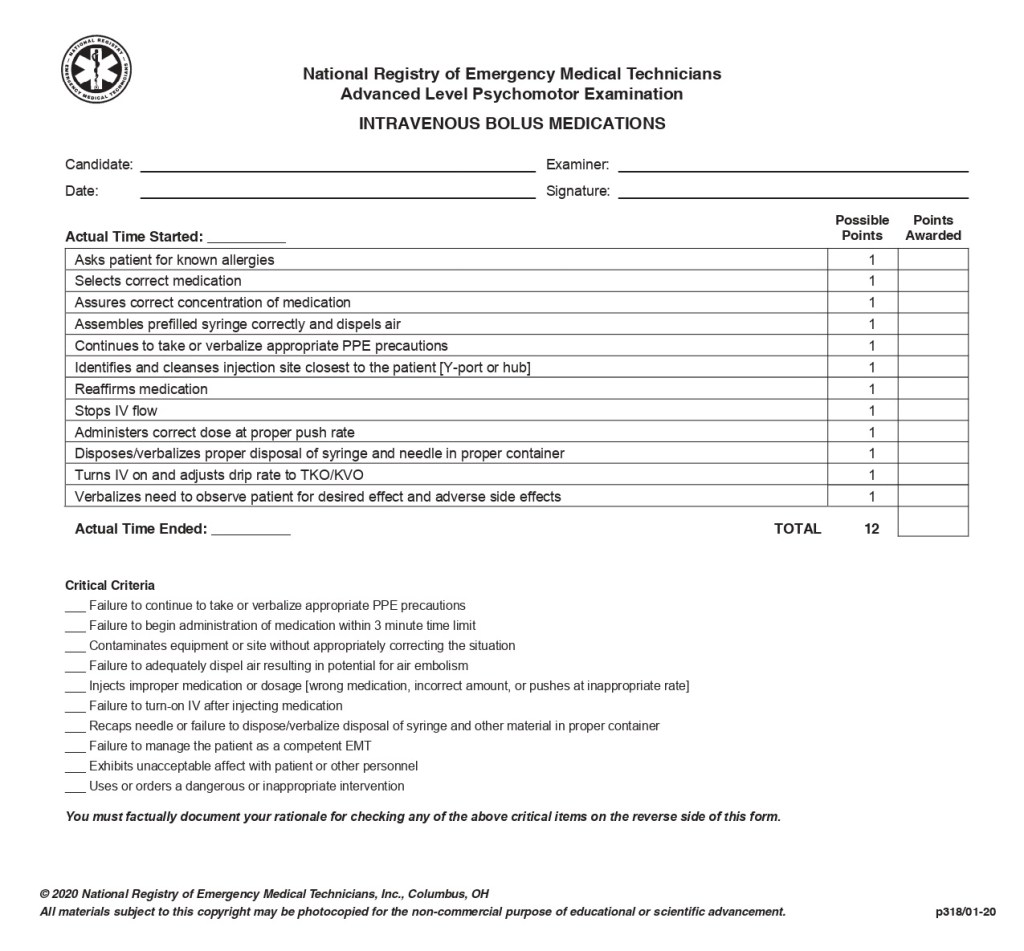
- Intravenous Bolus Medications
- This skill station requires you to administer an IV bolus medication via a pre-established IV. Most testing facilities will place this and the IV therapy skill together for ease. You will need to know what medications you can administer via IV as well as their indications, contraindications, and dosages. Ensure that you are using the correct medications throughout the skill station. YOU CAN NOT CHECK THE MEDICATION ENOUGH TIMES!!! Also, make sure to use an alcohol wipe to cleanse the IV port prior to administration of medication through it. Same as before, ensure that you dispose of the needle and medication vial appropriately. Following the medication administration, make sure you restart your IV fluid drip.
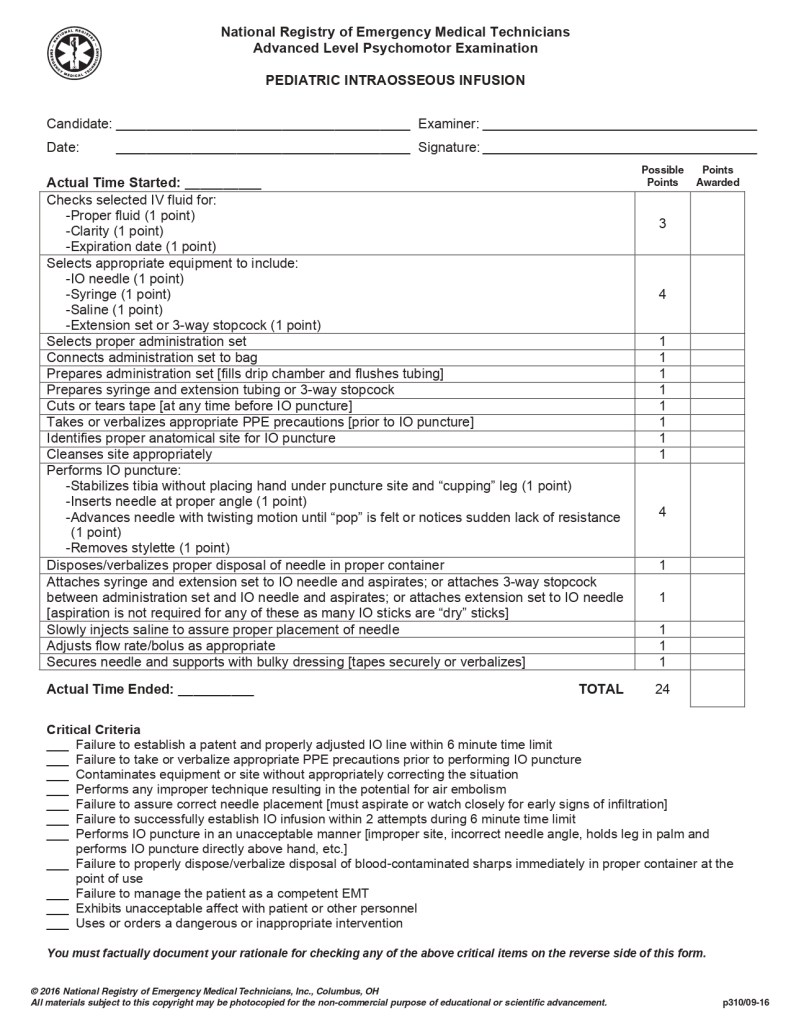
- Pediatric Intraosseous Infusion
- This skill station is very similar to the IV therapy station. When placing an IO, make sure you are selecting the correct insertion site. Also note, this procedure in the pre-hospital setting is reserved for unresponsive patients only. On a pediatric patient this is one finger below the proximal end of the tibia; there should be a flat surface at this location. You want to make sure the patient’s leg is slightly flexed and padding placed behind the leg. Do not hold behind the patient’s leg when doing this procedure, typically you will hold the leg near the area of the ankle. Same as before, make sure you use an “aseptic technique” to cleanse the area prior to puncture. Again, make sure you dispose of the needle as soon as it’s removed.
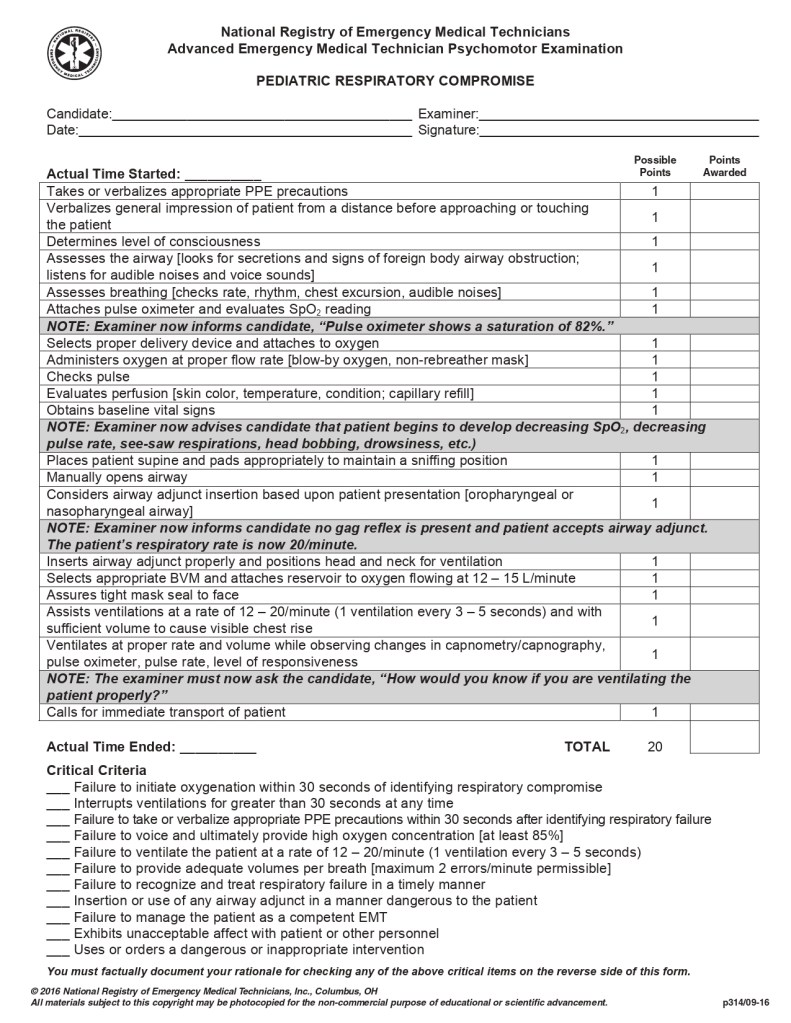
- Pediatric Respiratory Compromise
- This skill station is very similar to the adult oxygen administration scenarios mixed into one (Non-Rebreather and Bag Valve Mask);however, it is a pediatric patient. One of the biggest “catches” to this scenario is the early identification of respiratory compromise in this patient. When the patient begins to show signs of respiratory compromise, make sure you position the patient’s head into the “sniffing position” and pad any voids as necessary. For a child, padding behind the shoulder blades may be needed to ensure the airway is open and inline. The biggest different from the adult scenarios is that you need to verbalize the patient being placed on wavelength capnography and continuous monitoring.
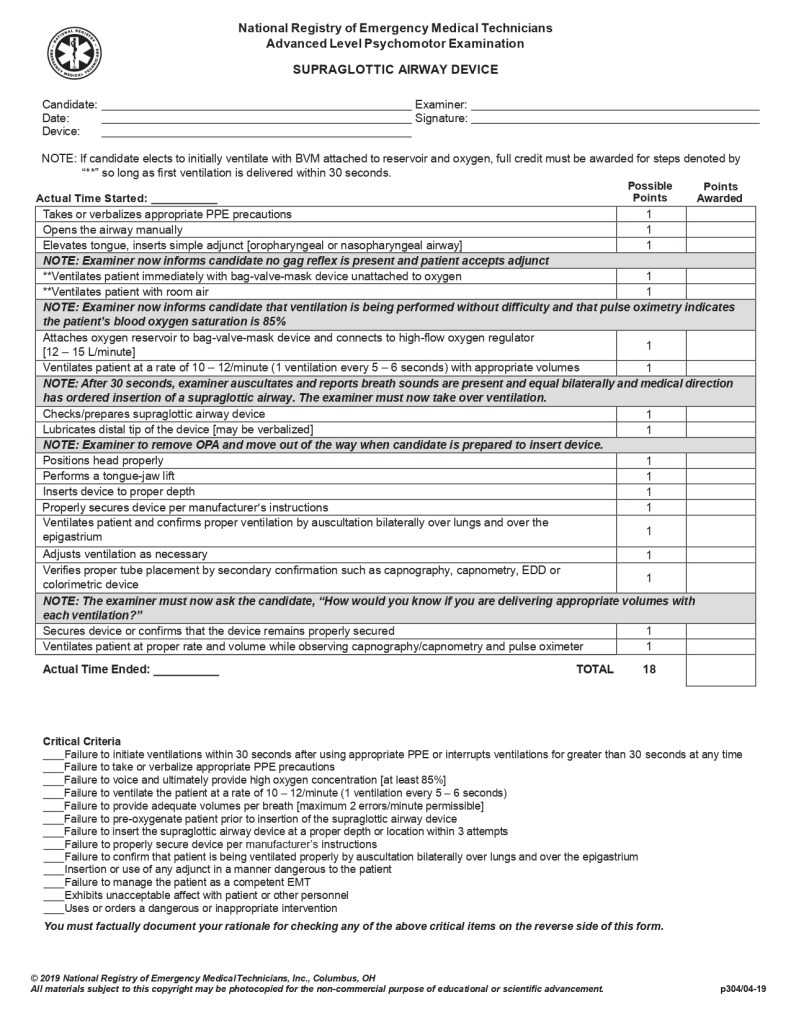
- Supraglottic Airway Device
- This skill is for the placement of a supraglottic airway. This can be any of the following devices: King LT, LMA, iGel, CombiTube, or any other “blind insertion” airway device. Depending on the site where you are testing, any combination of these airways is possible. Before you begin the scenario, you will have a couple of minutes to check your equipment. In the event that you don’t know how to use a specific device, this is your chance to inform the preceptor and they are required to show you how it functions. Before any advanced airway placement, you want to “pre-oxygenate” your patient. If you have been in EMS for more than a couple years, you will remember the wording of “hyper ventilate”; however, we no longer use this terminology. Make sure that before placing the device that you lubricate it to allow an easier placement and ensure correct placement. You will then auscultate both lungs and the gastric region to confirm correct placement, as well as establishing wavelength capnography with continuous monitoring. Same as with your Bag Valve Mask, make sure that your patient does not go over 30 seconds without ventilations.
For more information and examples of these skills stations, I recommend watching the video series by EMTprep on YouTube. For copies of these skill sheets, visit: https://emtprep.com/extra/nremt-exams/nremt-practical-exam-skill-sheets
If you have any questions about these skills stations, or need further explanation please reach out to me using the “Contact Us” page of this site.
