
Cerebrovascular Accidents (CVA) & Transient Ischemic Attacks (TIA)
Before we talk about anything else, we need to talk about the types of strokes.
There are two types of strokes, and they are pretty easy to tell apart (with the correct equipment).
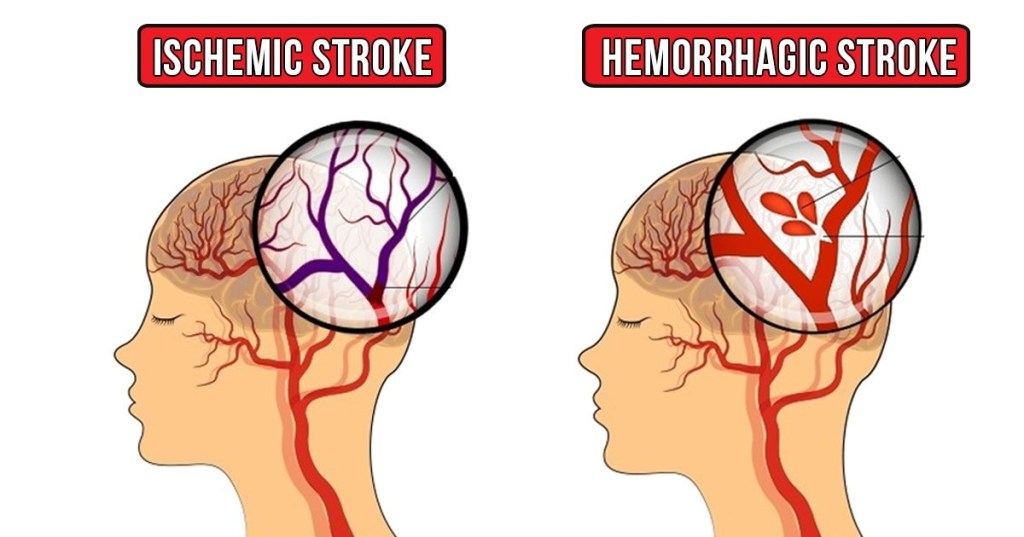
There are ischemic strokes, where a blood clot has formed and is occluding a large vessel to the brain, and there are hemorrhagic strokes where a large vessel has ruptured and the brain is not able to get the blood it requires.
Both types of strokes cause “ischemia” or death to the tissues of the brain. Over time, this damage will increase until complete cellular death has been achieved. This is why the saying “time is brain” is prevalent in the medical field, but we’ll get into that in a little bit.
So I said it pretty easy to tell the difference, right? Well, it is with a Computerized Tomography Scan, or “CT Scan” for us common folk. So how do you tell in the back of an ambulance? Well, you don’t…
All possible strokes should be treated equally until proven otherwise!!!
Now, typically hemorrhagic stroke patients will complain of the “worst headache of their life”, but this is not a definitive finding. Hemorrhagic strokes are very common following traumatic incidents, but again this is not definitive. The ONLY definitive way to tell the difference is you obtain a CT scan. So every hospital can do that, right?
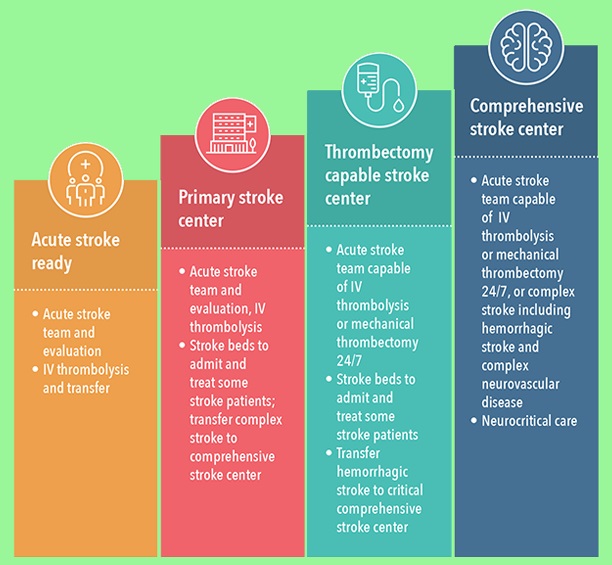
Well not necessarily…. So, for sake of simplicity, we are only going to cover primary and comprehenisive stroke centers today. Here in the Metro Atlanta area, we currently have three comprehensive stroke centers: Grady Memorial Hospital, Emory University (main), and Wellstar Kennestone Hospital. The rest of the hospitals in the area are primary stroke centers. But – what does that mean?
Well, a primary stroke center can administer a protein via IV called Tissue Plasminogen Activator, or more commonly known as “tPA”. This protein is a “clot buster” and is able to break apart blood clots. Useful for strokes, right? Well yes, if it is an ischemic stroke. Administration of this protein could be detrimental to the patient’s life in the event of a hemorrhagic stroke. That is why a CT scan is needed to be acquired to rule out a bleed, prior to the administration of tPA. So, all primary stroke centers can do this, so what does a comprehensive stroke center do?
Well, comprehensive stroke centers are able to perform thrombectomy, or surgical removal of the blood clot, and other brain surgeries such as placing a shunt to drain any blood in the cranial cavity. So why don’t we take all stroke patient’s directly to comprehensive centers? This boils down to the lack of availability. Metro Atlanta is a little spoiled, with so many hospitals, three of which being the highest level for stroke care. In other parts of the country, your nearest hospital may be over an hour away, and not even a comprehensive center. At the end of the day, you need to get these patient’s to the most appropriate care in the shortest amount of time. Sometimes that means taking them to a lower level center so the patient may be stabilized and later transferred out.
How do you know which facility to take the patient to? This all depends on time. The national standard time limit for tPA administration is currently up to four hours from the onset of symptoms. Yes, I said onset of symptoms, not your arrival time. Therefore your patient may be outside of the “tPA window” before you ever make it on scene. This is why documenting the time of onset of symptoms is so important, but we’ll get back to that in a little bit.
I would like to quote the lead neurosurgeon in the Metro Atlanta area: “if the patient is within the tPA window, AND CAN RECEIVE THE PRODUCT BEFORE THAT TIME EXPIRES, then take them to a primary stroke center if you believe the patient is having a CVA. If the patient is outside that window, then they need to be brought to a comprehensive center”. So what exactly does he mean by that? Well, if your patient began experiencing stroke symptoms three and a half hours ago, and you are 15 minutes from a primary stroke center, then take them there. However if the hospital isn’t going to be able to obtain a CT scan and administer tPA in that time frame, then they need to go to a comprehensive center. It’s as simple as that, right?
Unfortunately it isn’t always easy to determine if a patient is having a stroke, but we’ll talk stroke mimics and changes of mental status during a stroke in a future blog.
I do want to talk about a couple of very important things to keep in mind when it comes to stroke patients. First off, remember the “FAST” stroke scale.
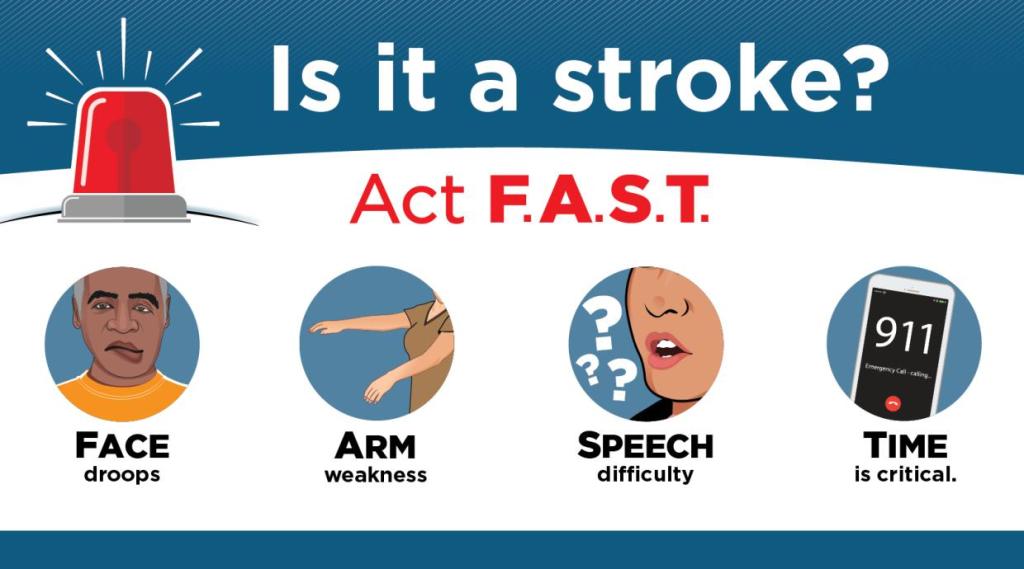
While this assessment isn’t definitive, it is a quick and easy tool to determine if a stroke is possible. So let’s briefly go over this scale:
1). Face – You want to check for any facial droop. Ask the patient to smile and “show you their teeth”. One side of the face could appear to be “melting” and become asymmetrical
2). Arm – Have your patient close their eyes (this is important) and raise their arms in front of them. Patient’s with a stroke could have one arm that falls after a short amount of time, or no control to an entire side of their body The patient needs to close their eyes during this test though, because they could over compensate for the irregularity and distort the findings
3). Speech – Have the patient repeat every EMT/Medic’s favorite saying “you can’t teach an old dog new tricks”, or something similar and easy to repeat. Stroke patients can have difficulty repeating simple phrases, or have slurred speech
4). And finally time – This one isn’t a finding, but serves as a reminder that “time is brain”. Remember that these patient’s brains are literally starving to death. The longer they go without blood supply, the more damage that will be done
Another VERY important topic in regards to stroke care is the information that needs to be obtained on scene. I know that most people in this field believe that we are here to treat our patients, and that’s it. However that is incorrect. We need to gather as much information about our patient’s as possible, including their medical history, medications, allergies, and yeah, their billing information. But again, that’s a topic for another day. So what information do we REALLY need for stroke patients in particular?
1). Patient’s Name
2). Date of Birth & Age (yes you need to be able to recall both)
3). Medical History
4). Medications; especially if any of them are blood thinners
5). Patient’s LAST KNOWN NORMAL!!!
6). Any other pertinent information for this patient (recent injuries, things like that)
7). Family Member’s Contact information (trust me, the neurologist will love you if you get this)
So, you’re transporting your stroke patient to the nearest facility and out of nowhere their signs completely subside. What gives? More than likely, the patient has experienced a Transient Ischemic Attack or “TIA”. This condition has unfortunately been incorrectly called a “mini stroke” in the past, when that couldn’t be further from the truth. A TIA is a full blown ischemic stroke, or sometimes vessel spasms. In reference to the ischemic TIA, the difference is that the blood clot has become dislodged and is no longer impeding blood flow to the brain. So why is this bad? Well, that clot didn’t just disappear. It is floating around somewhere in the body and could cause a secondary stroke, or a myocardial infarction (heart attack). Not to mention, this patient’s body is creating unneeded blood clots. These patients should be treated as a stroke patient until proven otherwise, regardless if symptoms have ceased. At the end of the day, the patient will receive a “stroke workup” to rule out a clot, and will also possibly be prescribed a blood thinner to combat any future clots.
So like I said, we don’t have enough time today to talk about stroke mimics, but that will be the topic of a future blog, so stay tuned!!! As always, thank you for taking time to read this blog, and I hope you were able to learn some new information on this very important topic.
