
Welcome back!!!
Let’s continue our talk on respiratory medications; Albuterol, Atrovent, Solu-Medrol, Magnesium Sulfate, & Epinephrine:
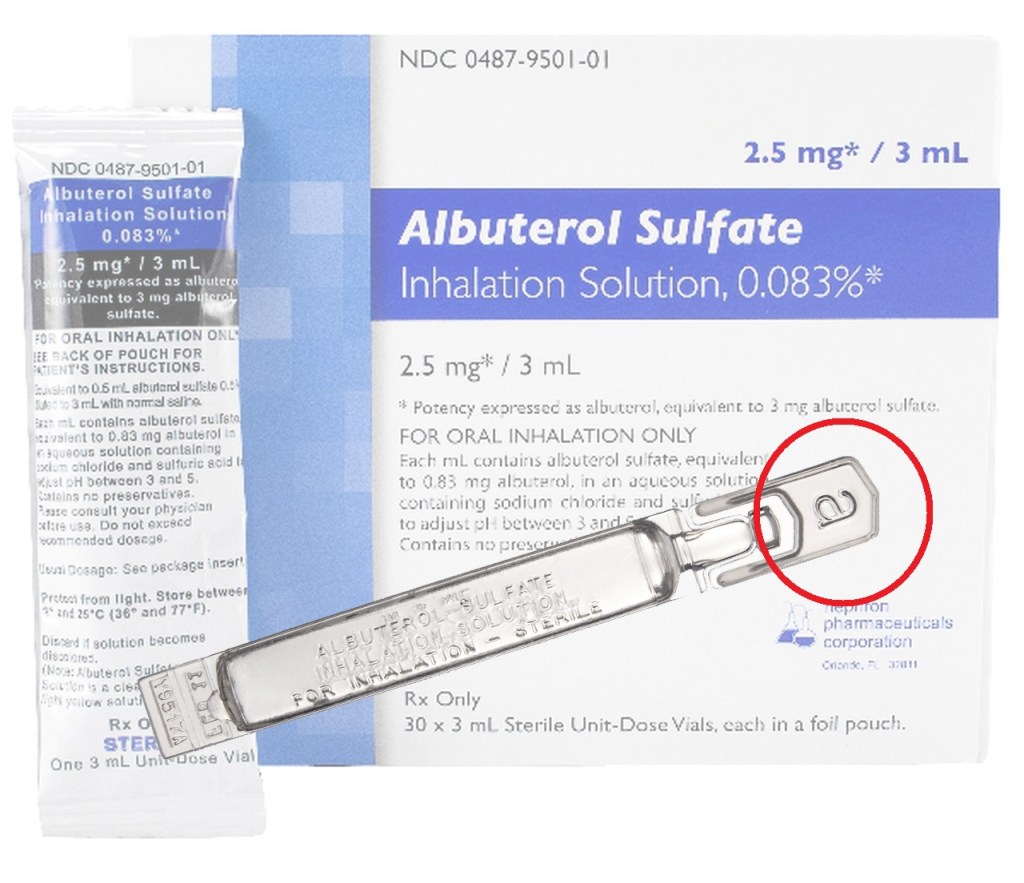
Albuterol: A Beta-2 Agonist that causes smooth muscle relaxation. The tissue that makes up the lungs is smooth muscle, so this medication is able to relax the lungs in the event that the muscle fibers are tightened and not allowing full movement. It does this by stimulating the adrenergic receptors of the sympathomimetic nervous system. In asthma patient’s albuterol is taken via meter-dosed inhaler (MDI), which is commonly taken prior to EMS arrival. EMT level providers are able to “assist” the patient to administer their medication if available. Albuterol is commonly administered in 2.5mg treatments via nebulizer, and can be given continuously throughout transport if needed. Albuterol is commonly sold in plastic tubes with the letter “A” at the top. Albuterol has a side effect of tachycardia, which can increase anxiety in patients who are experiencing an anxiety attack, and complaining of DIB. These patients will complain of being “unable to catch their breath, but their heart is racing”.

Atrovent: Also known as Ipratropium Bromide; stops interaction of acetylcholine at the receptor sites of the smooth muscles, causing bronchodilation. In short, this medication opens up the airways at the alveoli. This medication is typically administered at the dose of 0.5mg once via nebulizer. Atrovent is commonly sold in plastic tubes with the letter “I” at the top.

Methylprednisolone Sodium Succinate: Commonly known as “Solu-Medrol” is a corticosteroid that suppresses inflammation in the lungs. This medication works in conjunction with Albuterol to relax the smooth muscle of the lungs. In my opinion, this is the most interesting drugs that we can administer. The medication comes in a glass bottle and has two parts. The medication is actually a white powder that needs to be added to sterile water to be administered. Unlike other medication suspensions, this medication comes in a neat one-part bottle. To administer, you push down on the cap, which pushes a small rubber stopper to move and allow the two chambers of the container to mix. The medication is then mixed until dissolved, and then administered via an IV catheter. This medication is typically a single dose of 125mg for an adult patient. The issue with administration of this medication is that patient’s need to be tapered off of a steroid; therefore they will need to seek further medical treatment and possibly an Rx from the ER upon discharge. Another odd occurrence with this medication is its delayed reaction time. The average onset for Solu-Medrol is 1-2 hours; therefore you may not see your patient’s improvement from this medication in the field.
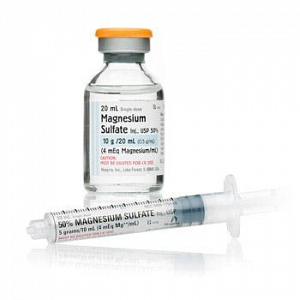
Magnesium Sulfate: Commonly known as “Mag”, this medication reduces muscle contractions and blocks peripheral neuromuscular transmission. This can cause bronchodilation after Albuterol has been administered. In other words, like Solu-Medrol, this medication relaxes the muscles of the lungs in conjunction with Albuterol. “Mag” can be a struggle to administer, due to it being an IV drip medication. “Mag” is administered at a rate of 2g over 10 or sometimes 20 minutes. Some services carry pre-made magnesium sulfate fluids, however most services require the paramedic to add the medication to a bag of Normal Saline for administration.

Epinephrine: Epinephrine is a “last ditch effort” when it comes to respiratory medications. Epinephrine is yet another smooth muscle relaxer that causes bronchodilation and reduces airway resistance. Epinephrine is also administered in allergic reactions due to its respiratory effects as well as its blockage of histamine. Epi is typically administered in two ways for a respiratory emergency, and that is a typical dose of 1:1000 0.3ml IM injection, or “Racemic” of 5ml (1%) in 5ml of normal saline. Racemic Epi can be in pre filled vials, or mixed by the paramedic, and is administered via Nebulizer over 10-20 minutes.
