Want to see how fast I can upset a bunch of EMS educators???
Let me show you…
SAMPLE HISTORY AND OPQRST ARE USELESS!
Now that I have your attention, let me explain. We are called to businesses and residences for other people’s emergencies. We are supposed to remain calm on scene and project that calmness on to our patients, their family members, and other bystanders on scene. So please tell me how walking into someone’s house, during one of the worst times of their lives, and rattling off a million questions (that they have most likely already answered), projects calmness?

IT DOESN’T!!!!
So, let’s break this down into a nice scenario for you. Say you are dispatched to a 40 year old male with stomach pain. When you get on scene, you introduce yourself and ask the patient what’s the reason they called 911. The patient tells you that he was mowing the grass when he had a sudden onset of right lower abdominal pain that radiates to his naval.
So, as you might have already deduced, this patient more than likely has appendicitis. But what else can you take away from what you know so far? The answer is a lot actually.
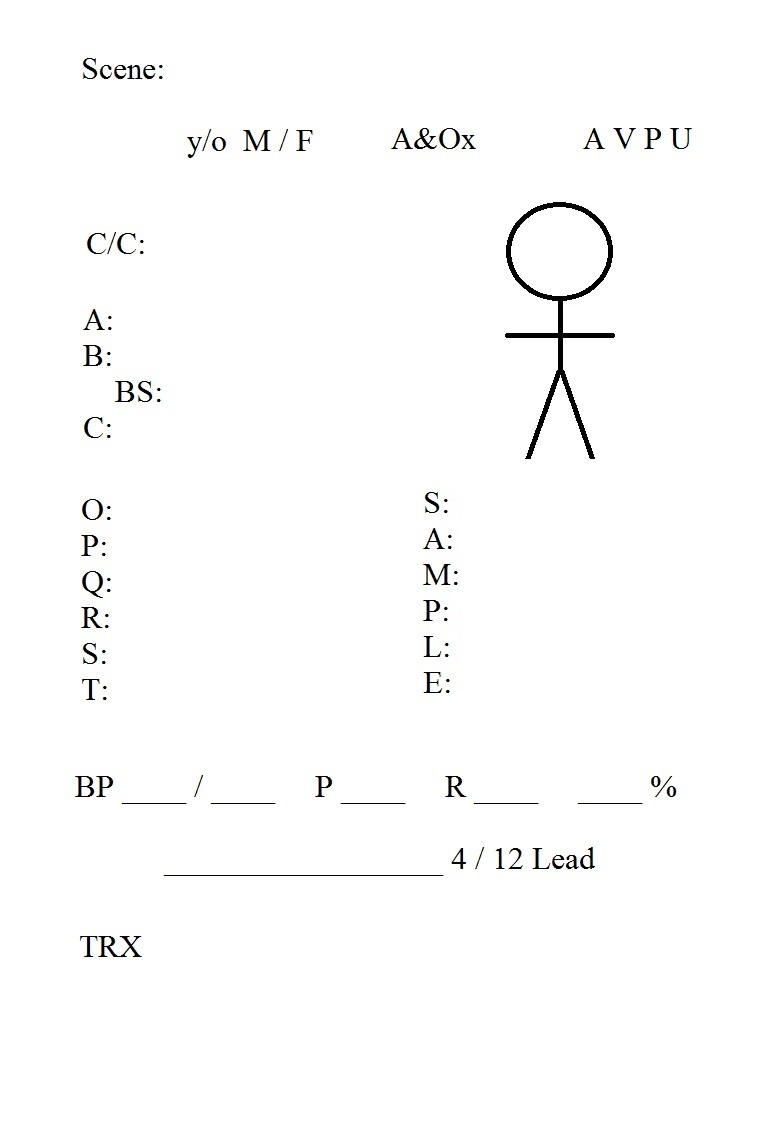
As I talked about in a previous post, I am a firm believer that the paramedic should have little to no physical contact with the patient if at all possible (depending on staffing, skill levels, etc.). If you have no clue what I’m talking about, please read my post titled “Running an Organized Cardiac Arrest”. Anyway, on scene I am typically standing away from the patient, delegating my crew to perform the required interventions, documenting what is taking place on scene, as well as recording any pertinent patient information. Organization is key here. I follow a template that has floated around the EMS community for a few years now, that I have tailored to my own needs. I have memorized the layout of this template and keep a small notebook in my pocket to write down all of the information needed.
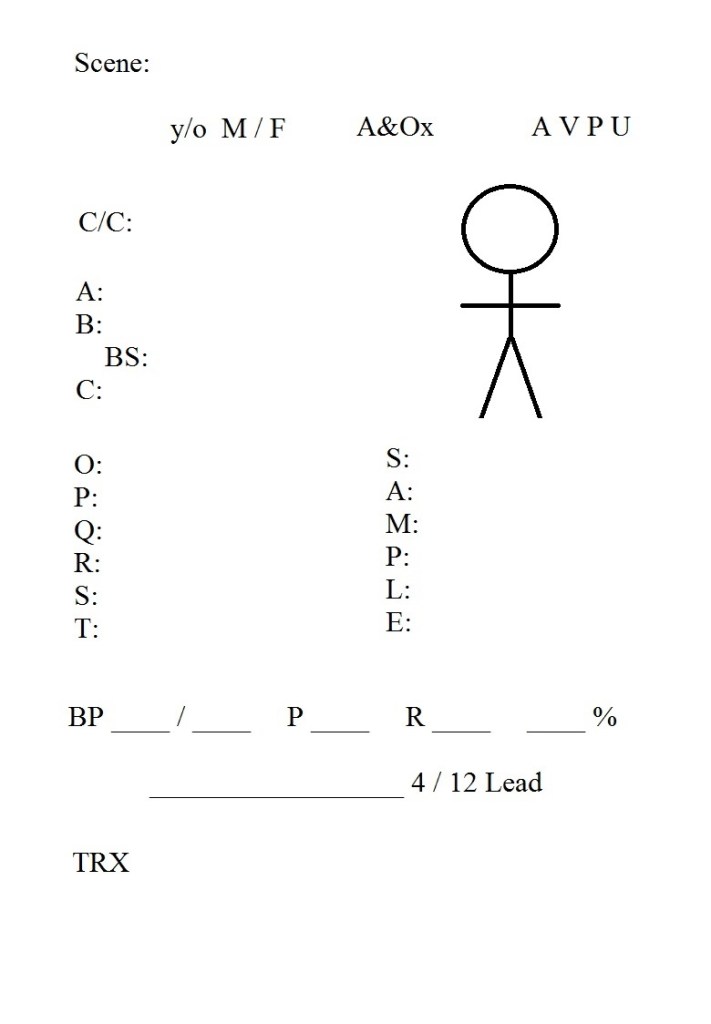
So if you refer back to our scenario, you can fill out about ¼ of this template just off of the dispatch information and your introduction. Next step is to delegate your team to get a baseline set of vitals. BOOM, now you have ½ of the information needed. Lastly you can ask the 4-5 remaining questions to secure ALL of the needed information. Can you see how this interaction could be perceived better than asking a bunch of questions right off the bat? It also gives the look that “everyone is doing something” and that there is no room for questioning by bystanders as to what is being done on scene.
I know this may seem minute and pointless, but try it out on your next call. I’m willing to bet that you, your crew, your patient, and any bystanders will be more at ease with this method. Just give it a shot.
After the call, you will have a nice written “summary” of the call along with any pertinent patient information you may need to do those ever lovely & tedious PCRs
